-
Home
-
Proper Patient Positioning Guidelines: Lithotomy Position
Proper Patient Positioning Guidelines: Lithotomy Position
June 21, 2018
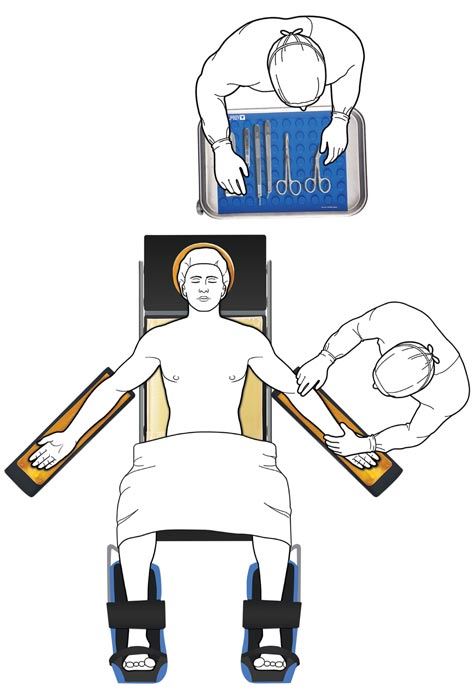
The supine position is the most commonly used position in surgery and has many variants; one such variant is the lithotomy position. The patient is placed on their back and legs are elevated at their hips. It is primarily used for procedures involving the perineum, pelvic organs, rectum, and genitalia.1 If the nursing assessment indicates limited range of hip motion due to arthritis, prosthesis, contractures or other conditions, patients may be placed into the position while awake so that they can participate in ensuring their comfort.
The head is supported by a patient positioning headrest like the AliGel Head Positioner or Single-Use Head Donuts. Ensuring the head and spine are aligned and the neck is in a neutral position. The patient’s arms are secured, using a strap such as AliMed Soft Precut Patient Positioning Straps, on padded arm boards to prevent crushing fingers and hands. The arm boards should be positioned at no more than 90 degrees, AliMed’s pivoting Armboard allows for incremental adjustments and to secure the board firmly in place. The legs are elevated, abducted, and supported in stirrups, such as the Ultrafin Stirrups, with the buttocks even with the lower break of the table. During elevation, the feet are held in one hand and the lower part of the leg in the other while the legs are slowly flexed. To prevent hip dislocation or muscle strain from the exaggerated range of motion, the legs should be raised and lowered slowly and simultaneously. At-risk pressure points vary depending upon the type of stirrups used, so perioperative nurses should pay particular attention to the femoral epicondyle, tibial condyles, and lateral and medial malleoli. The inner thighs and sacrum should be free of pressure, which should be accomplished via sufficient padding1, the Azure Sacral Pad is designed to relieve pressure on the sacrum. Correct placement of the safety strap is difficult in the lithotomy position. There is not a best practice for its placement; however, the safety restraint should not be placed over the patient’s chest or abdomen.
Modifications of the lithotomy position include low, standard, high, hemi, and exaggerated as dictated by how high the lower body is elevated for the procedure.1
- Low: The patient’s hips are flexed until the angle between the posterior surface of the patient’s thighs and the O.R. bed surface is 40 degrees to 60 degrees. The patient’s lower legs are parallel with the O.R. bed.2
- Standard: The patient’s hips are flexed until the angle between the posterior surface of the patient’s thighs and the O.R. bed surface is 80 degrees to 100 degrees. The patient’s lower legs are parallel with the O.R. bed.
- Hemi: The patient’s non-operative leg is positioned in standard lithotomy. The patient’s operative leg may be placed in traction.
- High: The patient’s hips are flexed until the angle between the posterior surface of the patient’s thighs and the O.R. bed surface is 110 degrees to 120 degrees. The patient’s lower legs are flexed.
- Exaggerated: The patient’s hips are flexed until the angle between the posterior surface of the patient’s thighs and the O.R. bed surface is 130 degrees to 150 degrees. The patient’s lower legs are almost vertical.
Following the procedure, the lower portion of the table is raided or replaced to align with the rest of the O.R. table. The patient’s legs are removed from the stirrups simultaneously, extended fully to prevent abduction of the hips and slowly lowered onto the table and the table strap, like the VeriClean Patient Safety Strap, is applied for safety.
References
- Burlingame B, Davidson J, Denholm B, et al. Guideline for positioning the patient. Guidelines for Perioperative Practice. 2017;1. DOI: 10.6015/psrp.17.01.e1.
- Rowen L, Hunt D, Johnson KL. Managing obese patients in the OR. OR Nurse. 2012; 6(2):26-36.